| There is a moment that happens regularly in fetal cardiology referrals. A first-trimester scan shows an elevated nuchal translucency. The karyotype comes back normal. And somewhere along the way, the worry quietly dissolves, as though the chromosomes have spoken for the heart as well. They have not. |
1. What NT Is Actually Measuring
Nuchal translucency reflects the accumulation of fluid in the subcutaneous space behind the fetal neck, measured between 11 and 13+6 weeks of gestation. It became widely known as a screening marker for chromosomal anomalies, particularly trisomy 21, and that association is real and well-established.
But NT is not a chromosomal marker alone. Understanding what drives the fluid to accumulate in the first place is key to understanding why the heart is so often involved.
Three mechanisms link elevated NT to cardiac pathology. Each works independently, and each points back to the heart as a potential source, not merely a bystander.
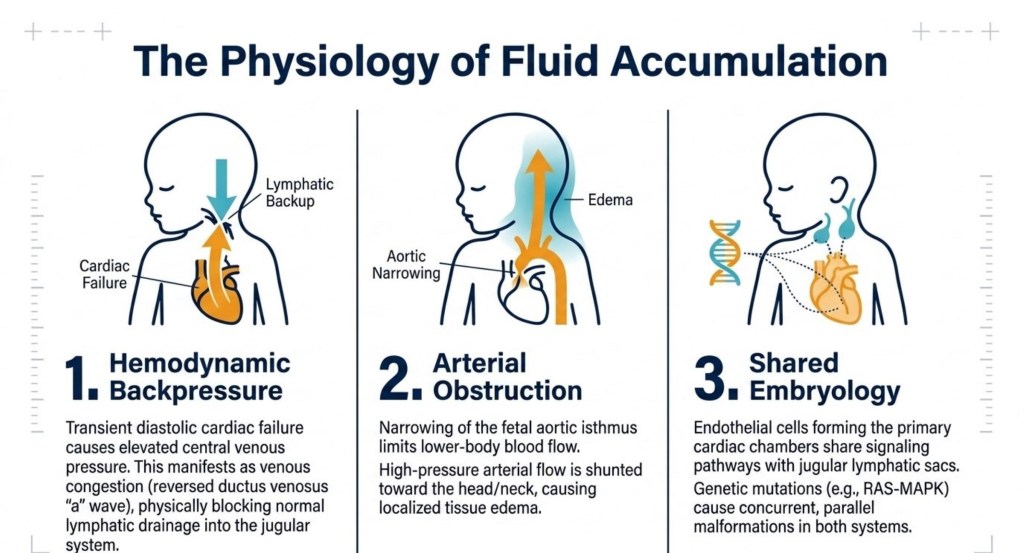
Figure: The three pathways: haemodynamic backpressure from cardiac failure; arterial obstruction redirecting flow toward the head and neck; and shared embryological signalling between cardiac chambers and jugular lymphatic sacs.
Haemodynamic backpressure
Transient diastolic cardiac failure can raise central venous pressure and impede normal lymphatic drainage into the jugular system. As drainage is blocked, fluid accumulates behind the fetal neck.
Arterial obstruction
Narrowing of the fetal aortic isthmus can reduce blood flow to the lower body. The resulting redistribution of high-pressure flow toward the head and neck may produce localised tissue oedema.
Shared embryology
The endothelial cells that form the cardiac chambers share developmental signalling pathways with the jugular lymphatic sacs. A single genetic variant can therefore disrupt both systems simultaneously, leading to concurrent malformations.
NT is therefore a marker of abnormal lymphatic drainage, altered cardiac function, and disrupted haemodynamic flow in early fetal life. The heart is not a bystander in this process. It is often the cause.
2. The Cardiac Risk That Persists After a Normal Karyotype
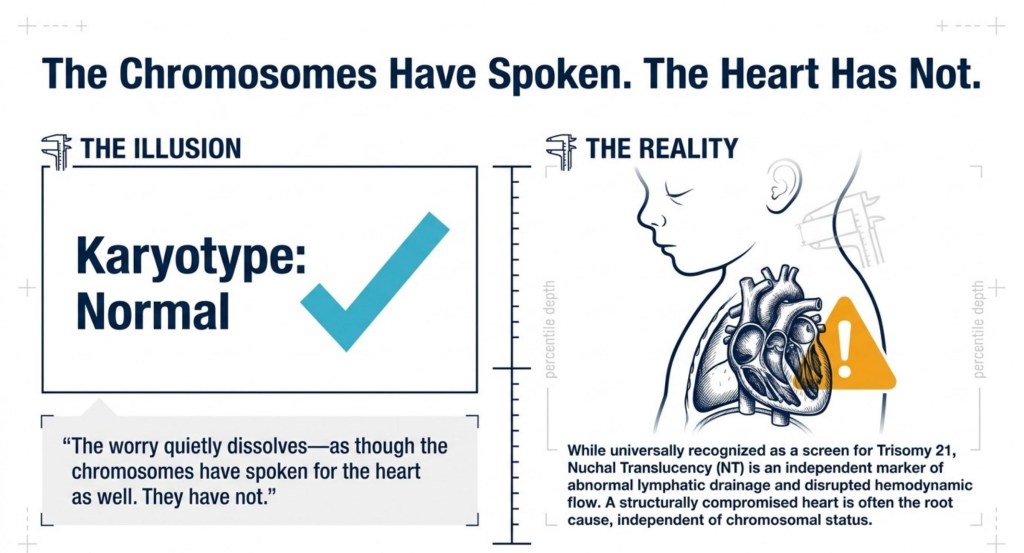
Figure: The clinical disconnect: a normal karyotype result addresses chromosomes only. It does not evaluate cardiac structure, haemodynamic function, or lymphatic drainage.
Once a chromosomal abnormality has been excluded, the background risk of congenital heart disease in the general population sits at roughly 0.8 to 1%. An elevated NT changes that number substantially, and the change is proportional to how elevated the NT is.
⚠️ The risk is proportional, not binary. There is no sudden jump at one specific threshold. Risk escalates continuously from 3.0 mm upward. This matters for the 3.0–3.4 mm group, who are often not referred.
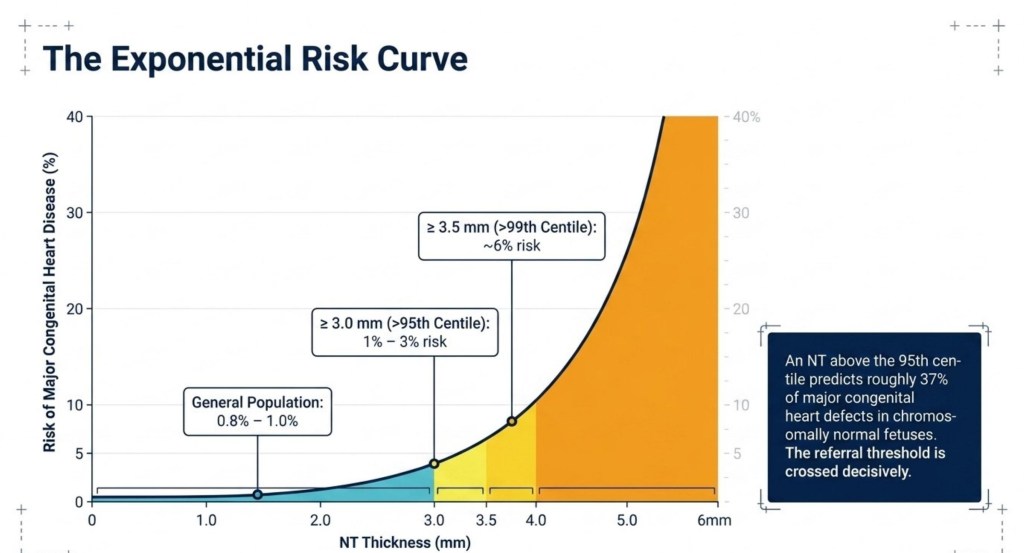
Figure: The exponential risk curve. Risk accelerates sharply above 3.0 mm. NT above the 95th centile predicts approximately 37% of major CHD in chromosomally normal fetuses (Sotiriadis et al., 2013).
| KEY FINDING A pooled analysis of 637 cases of CHD with known karyotype found that among chromosomally normal fetuses, nearly 23% had an NT of 3.5 mm or above. The elevated NT was distributed across all subtypes of CHD with no predilection for any single group. |
Elevated NT does not flag a particular cardiac diagnosis. It flags cardiac risk across the full spectrum.
3. The Diagnostic Window That Opens Earlier
There is a second, often overlooked benefit to taking the NT-cardiac connection seriously: timing of diagnosis. In chromosomally normal fetuses with an NT of 3.5 mm or above, the mean gestational age at diagnosis of CHD was 16.1 weeks, compared to 22.1 weeks in those with a normal NT.
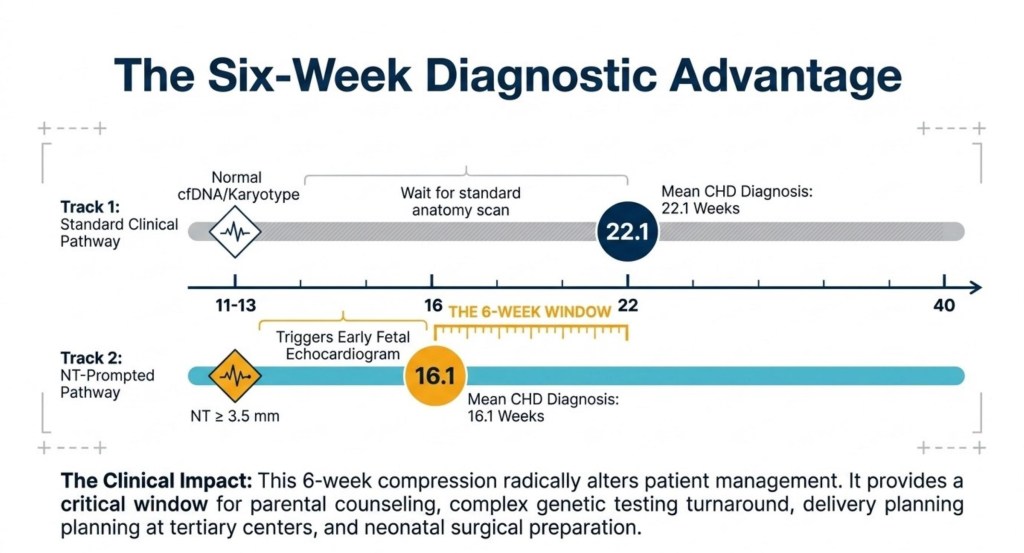
Figure: Two clinical pathways compared. NT-prompted echocardiography shifts mean CHD diagnosis from 22.1 weeks to 16.1 weeks, providing a six-week window for counselling, genetic testing, and delivery planning.
This six-week compression has real clinical consequences. The timeline below shows what can be achieved in that window:
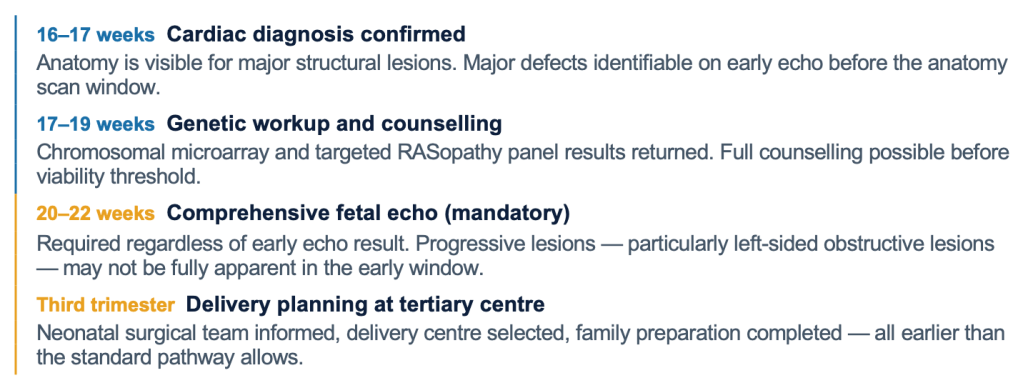
| ✔ Important note on early echo: A clear scan at 16–18 weeks does not cancel the requirement for a comprehensive fetal echocardiogram at 20–22 weeks. Progressive lesions such as coarctation of the aorta may not be apparent in the early window and require the later scan for definitive assessment. |
4. The Lesions to Keep in Mind
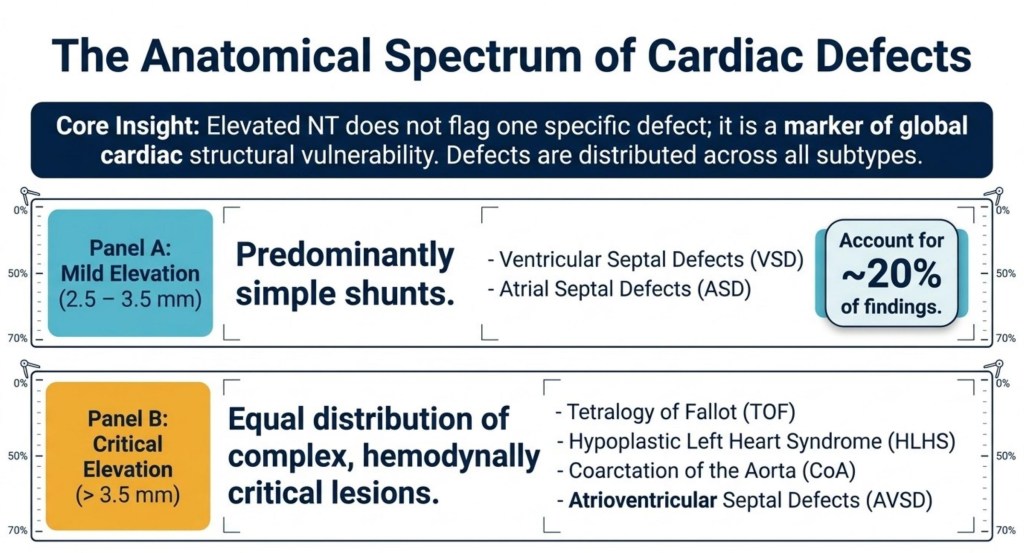
Figure: The spectrum of associated cardiac defects stratified by NT elevation. Mild elevation (2.5–3.5 mm): predominantly simple shunts. Critical elevation (> 3.5 mm): equal distribution of haemodynamically significant lesions, including HLHS, coarctation, TOF, and AVSD.
| ⚠️ Do not assume mild lesions. Hypoplastic left heart syndrome and coarctation of the aorta both appear in the elevated NT context. The elevated NT is sometimes the first — and only — early signal of a haemodynamically critical lesion. |
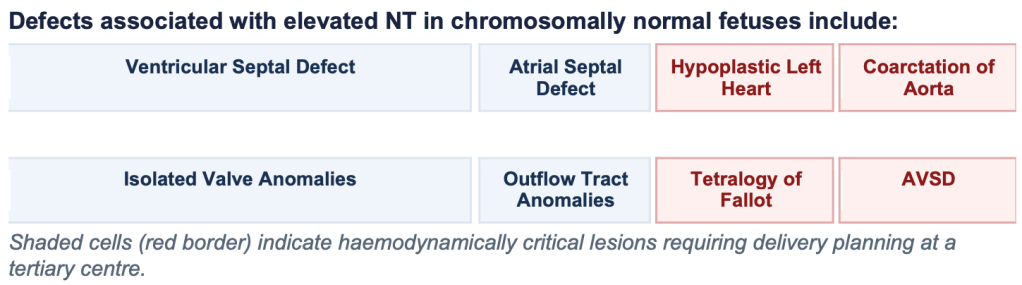
Defects associated with elevated NT in chromosomally normal fetuses include:
5. What the Guidelines Recommend
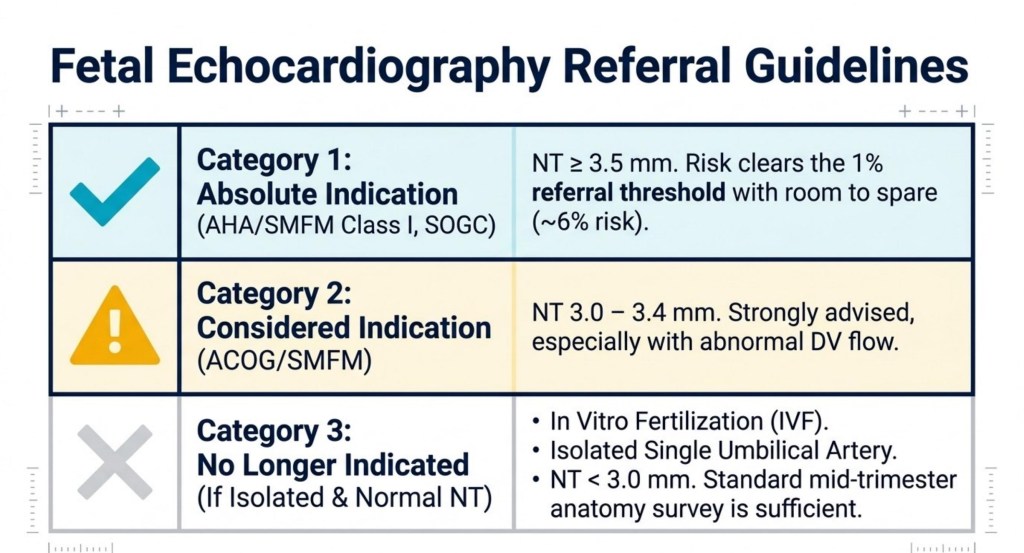
Figure: Current referral framework. Category 1 (absolute): NT ≥ 3.5 mm. Category 2 (considered): NT 3.0–3.4 mm, especially with abnormal DV flow. Normal NT with no additional risk factors: standard mid-trimester anatomy scan.
The 2023 updated guidelines from the American Society of Echocardiography are clear on this point. Fetal echocardiography is recommended when NT is 3.5 mm or above, and should be considered when NT is between 3.0 and 3.5 mm.
| 📋 The underlying threshold principle: Fetal echocardiography is warranted when the estimated risk of CHD exceeds approximately three times the background population risk, corresponding to roughly 1%. An NT of 3.5 mm decisively crosses that threshold. The ductus venosus waveform is the key adjunct in the 3.0–3.4 mm grey zone. |
6. What Comes After the Diagnosis
The prognosis for CHD identified in the context of elevated NT is not the same as for CHD identified through standard screening. The mortality data show a consistent and widening gap.
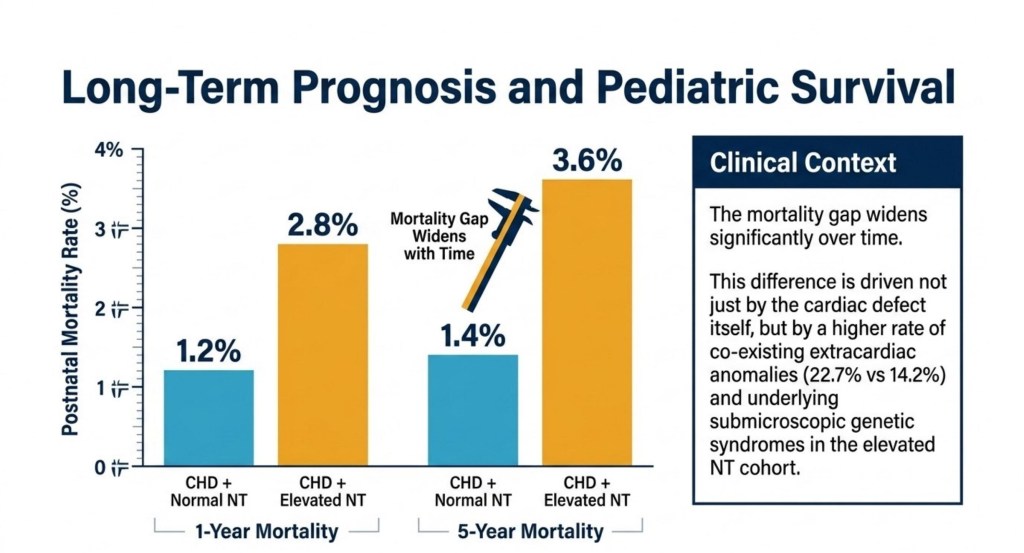
Figure: Postnatal mortality at one and five years for CHD with normal versus elevated NT. The gap widens over time, driven by co-existing extracardiac anomalies and submicroscopic genetic syndromes that standard karyotyping does not detect.
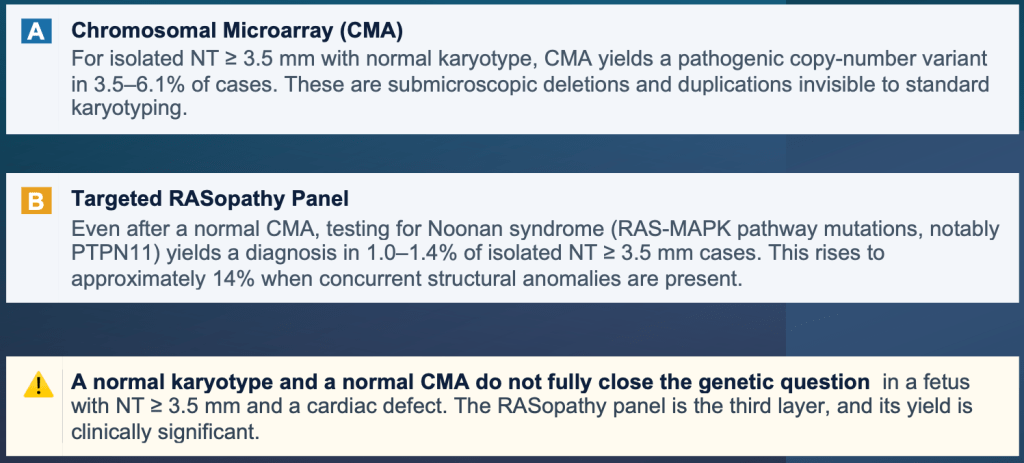
This difference is not driven by the cardiac defect in isolation. It reflects the broader genetic and structural burden that elevated NT represents. Two additional investigations have a meaningful yield in this population, even after a normal conventional karyotype:
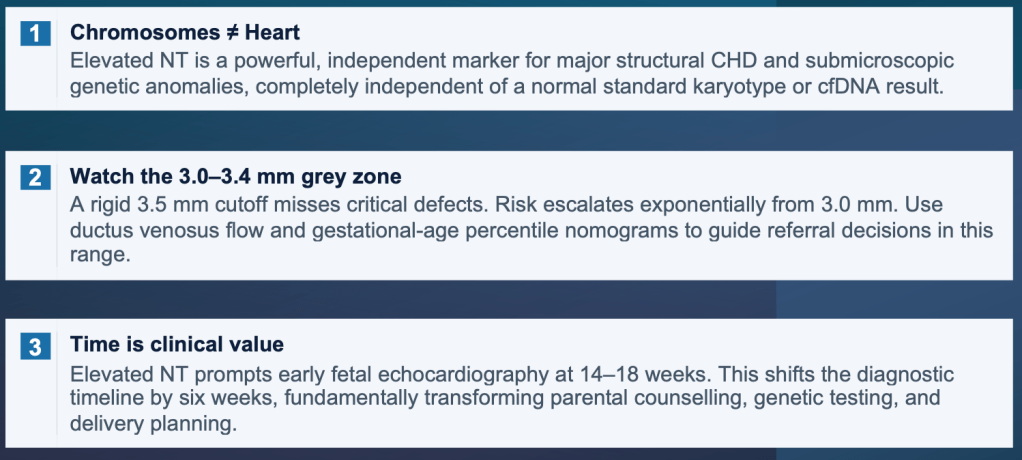
7. The Practical Point
Normal chromosomes do not equal a normal heart. Elevated NT is an independent cardiac risk marker, and the data supporting fetal echocardiography in this setting have been accumulating for two decades. The referral conversation is worth having, and worth having early.
| A note on the mid-trimester scan A normal NT in a chromosomally normal fetus does not eliminate the need for a good cardiac view at the mid-trimester anatomy scan. An elevated NT that returns a normal karyotype has not been cleared; it has answered only one question out of several. The fetal heart deserves its own assessment, on its own terms, by the 20th week at the latest. |
References
Sotiriadis A et al. Ultrasound Obstet Gynecol 2013 • Smrcek JM et al. Am J Obstet Gynecol 2005 • American Society of Echocardiography: Guidelines for Fetal Echocardiography 2023
