The Fetal Cardiac Axis
Normal range, measurement technique, abnormal axis associations, and clinical decision pathway. A practical reference for obstetricians, sonographers, and MFM clinicians.
Open Interactive Guide →Opens in a new tab · No login required
The cardiac axis appears in every major fetal echocardiography guideline, sits in plain sight on every four-chamber view, and takes approximately ten seconds to assess. Yet in routine practice, it is frequently noted as an afterthought — or skipped entirely.
This is worth correcting.
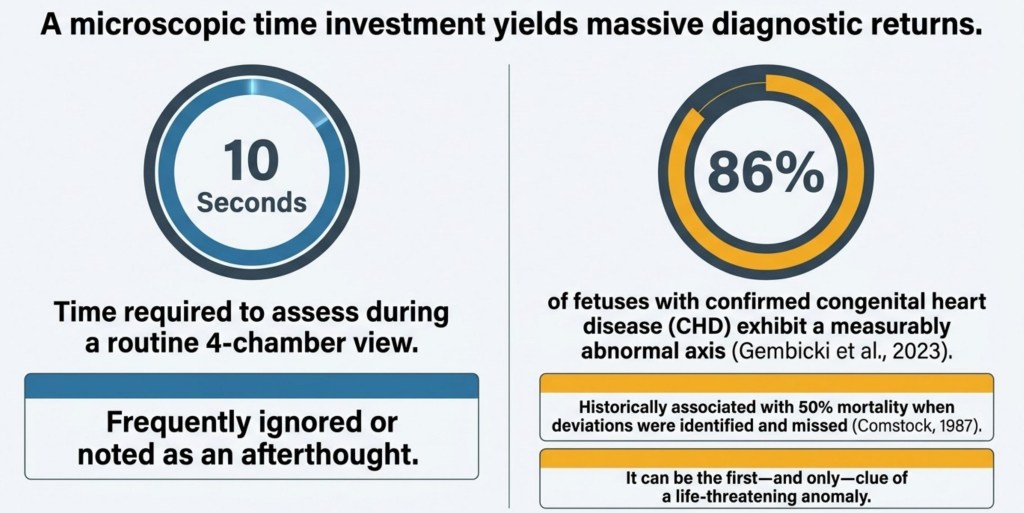
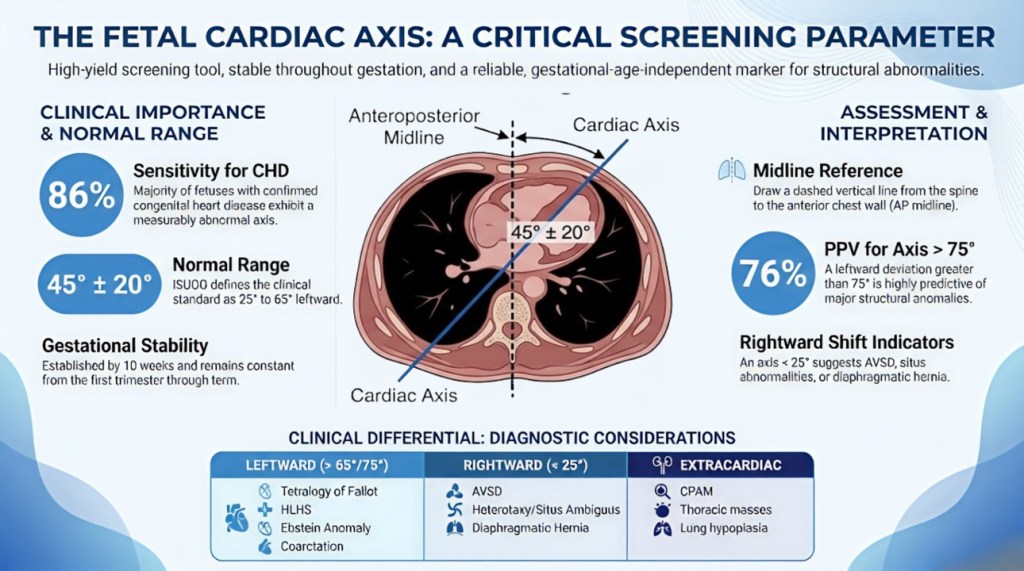
An abnormal cardiac axis can be the first — and sometimes only — sign of a significant cardiac or thoracic abnormality visible on a routine scan. When axis deviations were identified and missed in Comstock’s original 1987 cohort, mortality in those cases reached 50%. More recently, the FINE-based study by Gembicki et al. (2023) found that approximately 86% of fetuses with confirmed congenital heart disease had a measurably abnormal axis.
The ratio is difficult to ignore: ten seconds of assessment time, with diagnostic returns that can change the entire management of a pregnancy.
What the Cardiac Axis Is
The cardiac axis describes the angle that the interventricular septum (IVS) makes with a reference line drawn from the spine to the anterior chest wall, measured on the four-chamber view. In a structurally normal fetus, the heart sits predominantly in the left chest with the apex pointing leftward and anteriorly. This orientation is consistent from the first trimester through to term.
One important clarification before measuring:
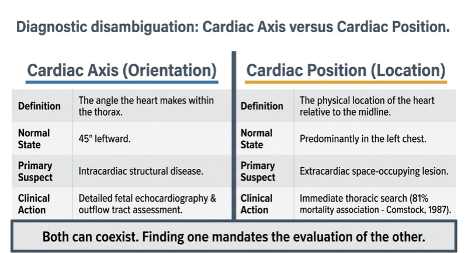
Cardiac axis (orientation) and cardiac position (location) are not the same findings and do not have the same clinical implications. Both can coexist — finding one mandates evaluation of the other.
The cardiac axis is the angle the heart makes within the thorax. The cardiac position is where the posterior border of the heart sits relative to the midline. An abnormal axis most often reflects primary cardiac structural disease. An abnormal position most often reflects a space-occupying thoracic lesion displacing the heart mechanically. Comstock (1987) found that abnormal position carried 81% mortality in her series — the reflex should be an immediate thoracic search.
How to Measure It
The measurement is made entirely within the standard four-chamber view:
- Freeze the image in mid-diastole at the level of the atrioventricular valves.
- Draw a reference line from the midpoint of the spine to the anterior chest wall (the anteroposterior midline).
- Draw a second line along the long axis of the interventricular septum.
- Measure the angle between these two lines on the left side of the thorax.
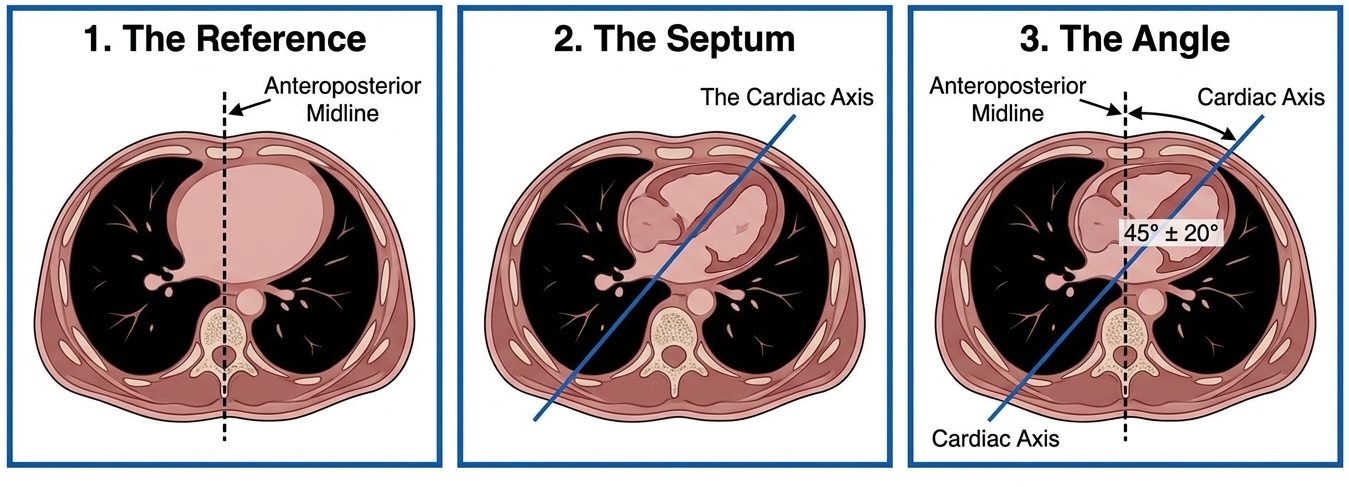
The result is reported as degrees of leftward deviation. Most ultrasound platforms support a direct on-screen angle measurement. Smith et al. (1995) confirmed that on-screen electronic measurement and direct protractor measurement produce statistically equivalent results.
The most common pitfall is an oblique scan plane — this artificially shifts the apparent axis and can generate both false positives and false negatives. Always confirm that the spine, ribs, and cardiac structures are at the same level in the same image before recording a measurement.
The Normal Range

Three reference ranges appear in the literature, and it helps to understand why they differ:
- Comstock (1987): 22° to 75° — the full observed range from a prospective cohort of 183 normal fetuses. This is the outermost boundary of normal data, not a clinical action threshold.
- ISUOG Guidelines: 25° to 65° (45° ± 20°) — the 2-SD range adopted for routine clinical screening. Values outside this range warrant further assessment.
- Greater than 75° (Smith et al. threshold) — in a prospective cohort of approximately 41,500 fetuses, an axis exceeding 75° had a positive predictive value of 76% for structural abnormality (Smith et al., 1995, PMID: 7824228).
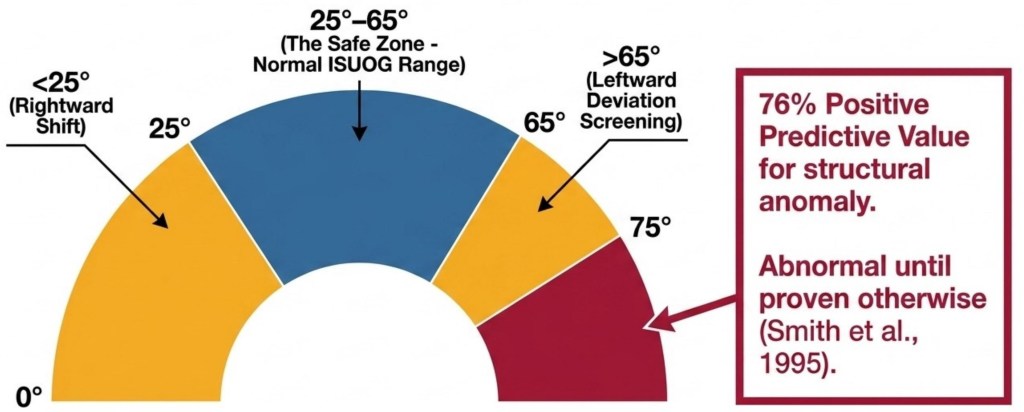
The diagnostic spectrum of the fetal cardiac axis. Any axis outside 25° to 65° is the screening threshold for referral. An axis greater than 75° carries a 76% PPV for structural anomaly and is abnormal until proven otherwise.
Leftward Axis Deviation (greater than 65°)
Excessive leftward rotation is the most common direction of abnormal deviation and is most strongly associated with conotruncal anomalies.
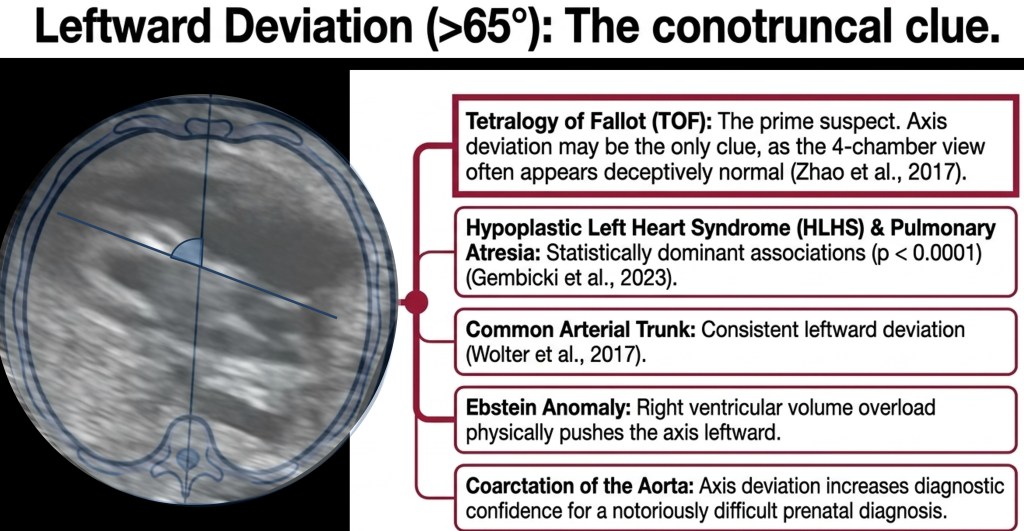
The single most important point for routine scanning is this: Tetralogy of Fallot, common arterial trunk, and several other conotruncal lesions frequently present with a deceptively normal four-chamber view. A deviated axis may be the only visible abnormality at the time of the anomaly scan. This is precisely why measuring the axis belongs in routine cardiac screening.
Diagnoses associated with leftward deviation (greater than 65°):
- Tetralogy of Fallot — axis deviation reaches statistical significance at p < 0.0001 (Gembicki et al., 2023).
- Common arterial trunk (truncus arteriosus) — conotruncal association.
- Hypoplastic left heart syndrome (HLHS) — p < 0.0001.
- Pulmonary atresia — p < 0.0001.
- Ebstein anomaly — RV volume overload mechanically rotates the axis leftward.
- Coarctation of the aorta — axis deviation is a useful corroborating finding in a diagnosis that is often subtle.
- Absent pulmonary valve syndrome — p 0.001 to 0.01.
Rightward Axis Deviation (less than 25°)
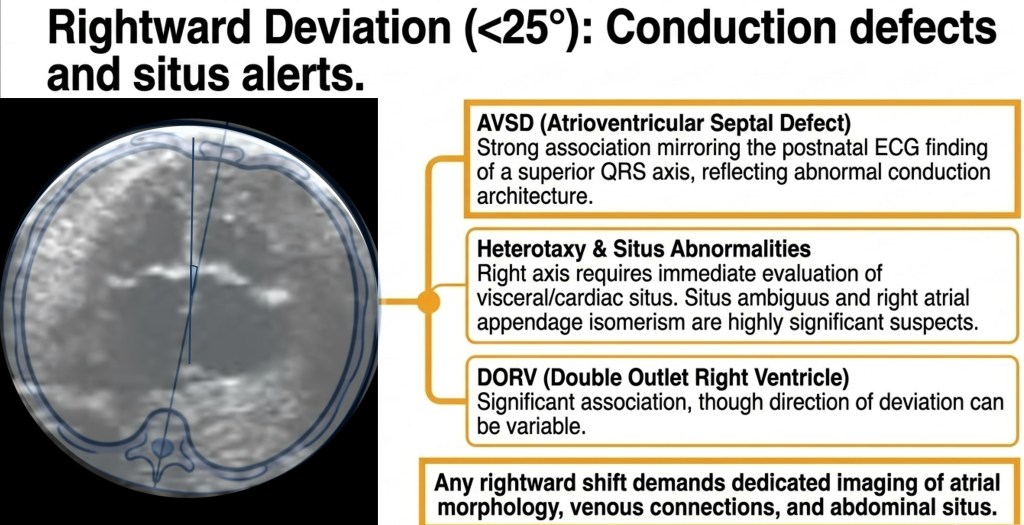
Rightward axis deviation (less than 25°) has a distinct set of associations. Any rightward shift demands dedicated imaging of atrial morphology, venous connections, and abdominal situs.
Rightward deviation carries a different differential and is less common, but arguably more alarming when encountered. The primary concern is heterotaxy.
Key associations:
- AVSD — consistent with the postnatal ECG finding of superior QRS axis, reflecting abnormal conduction architecture.
- Situs ambiguus and right atrial appendage isomerism — highly significant deviation (p 0.0001 to 0.001).
- DORV — variable direction but statistically significant association.
- TGA — wide axis range; the four-chamber view is frequently normal.
Any rightward axis deviation demands systematic assessment of abdominal situs, atrial morphology, and venous connections. Heterotaxy carries complex multisystem implications that extend well beyond the cardiac anatomy.
Extracardiac Causes: The Thorax Must Be Examined
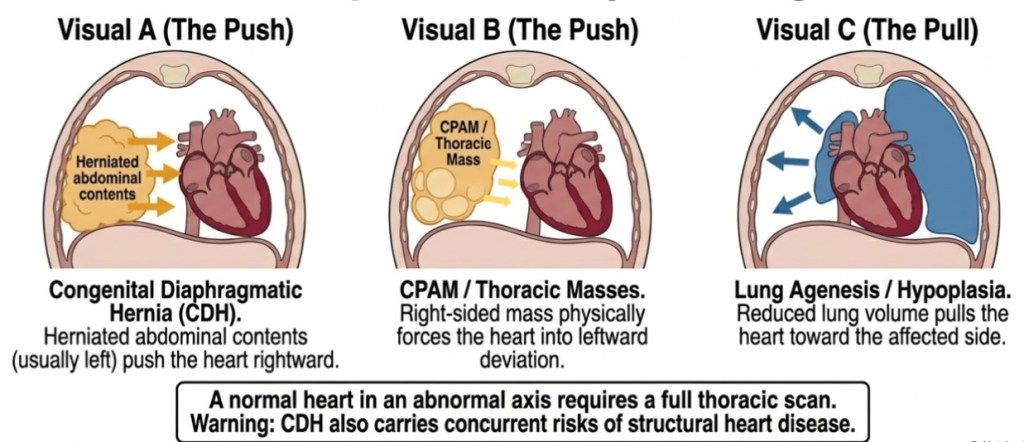
Three mechanisms by which extracardiac pathology displaces the cardiac axis: CDH (push from left hernia contents), CPAM or thoracic mass (push from the right), and lung agenesis/hypoplasia (pull toward the affected side). Normal cardiac anatomy does not exclude these diagnoses.
Not every axis abnormality is cardiac in origin. Space-occupying thoracic lesions displace the heart mechanically and produce a secondary axis deviation that has nothing to do with cardiac structure.
- Congenital diaphragmatic hernia (CDH) — herniated abdominal contents (usually left-sided) push the heart rightward. Even when CDH is the primary diagnosis, full cardiac evaluation remains important: CHD co-occurs in up to 31% of CDH cases.
- CPAM and other thoracic masses — a right-sided mass physically forces the heart into leftward deviation. Axis deviation from thoracic mass was statistically significant in the FINE dataset (p 0.001 to 0.01).
- Lung agenesis or hypoplasia — reduced lung volume pulls the heart toward the affected side. This is passive displacement, not a structural cardiac abnormality.
| Important A structurally normal heart in an abnormal axis is not a reason for reassurance in the absence of a clear extracardiac explanation. It remains an indication for careful follow-up and thoracic assessment. |
Putting It Together: The Diagnostic Differential
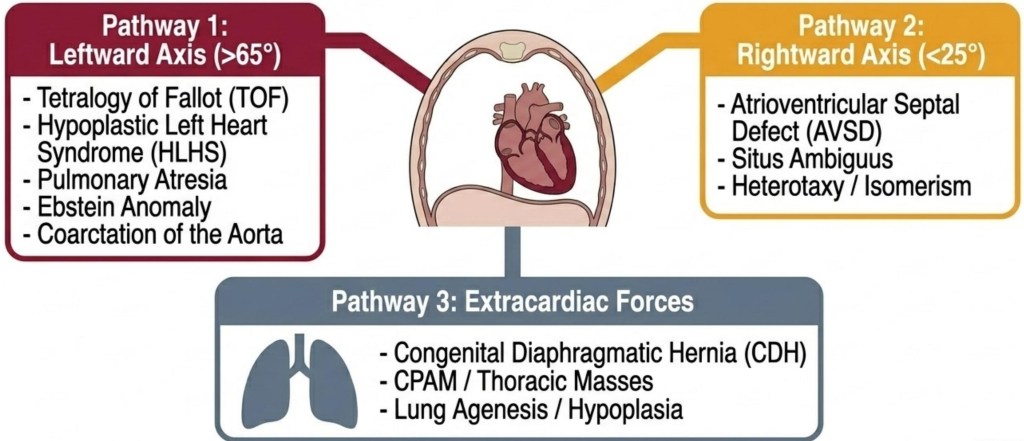
The Axis Outlier Map — a unified diagnostic differential covering leftward deviation (>65°), rightward deviation (<25°), and extracardiac forces. Any abnormal axis should be mapped against all three pathways.
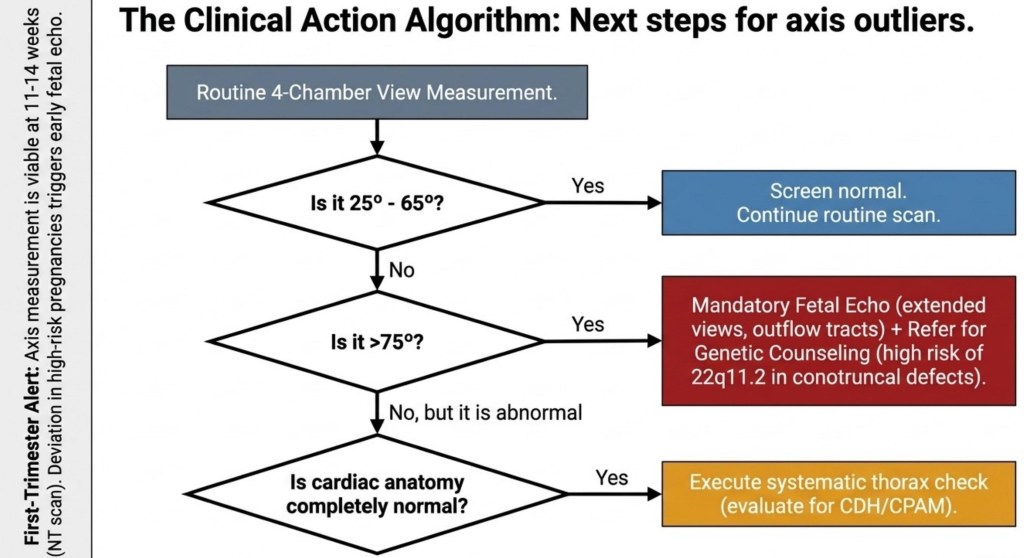
The clinical action algorithm for an abnormal axis. Note the first-trimester alert: axis measurement is viable from 11 to 14 weeks, and deviation at the NT scan in a high-risk pregnancy triggers early fetal echo.
The clinical response is consistent regardless of which direction the axis is abnormal:
- Axis outside 25° to 65° — examine the thorax for extracardiac pathology first. If the thorax is clear, attempt outflow tract and three-vessel trachea views on the same visit. Refer for formal fetal echocardiography.
- Axis greater than 75° — mandatory formal fetal echo with extended views (LVOT, RVOT, three-vessel trachea view, ductal and aortic arches, venous connections). Where a conotruncal lesion is confirmed, discuss 22q11.2 microarray analysis.
- Rightward axis — systematic assessment of abdominal and atrial situs. Atrial morphology, IVC laterality, and pulmonary venous connections take priority.
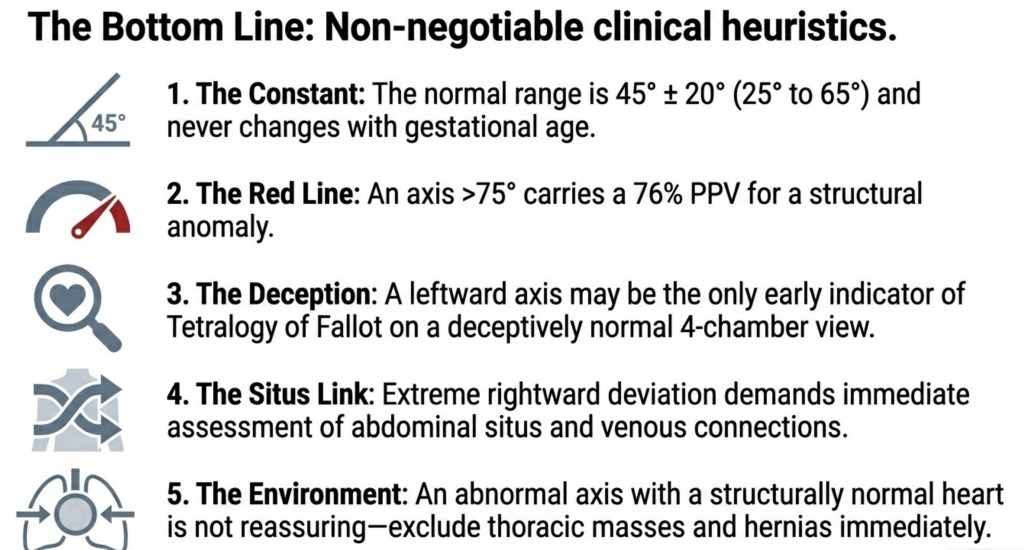
Five non-negotiable clinical principles for the fetal cardiac axis. Based on Comstock (1987), ISUOG guidelines, Smith et al. (1995), and the FINE dataset (Gembicki et al., 2023).
- The Constant: The normal range is 45° ± 20° (25° to 65°) and does not change with gestational age.
- The Red Line: An axis greater than 75° carries a 76% positive predictive value for structural anomaly. It is abnormal until proven otherwise.
- The Deception: In Tetralogy of Fallot, a deviated axis on a normal-looking four-chamber view may be the only early sign. The outflow tracts are where the diagnosis lives.
- The Situs Link: Extreme rightward deviation demands immediate assessment of abdominal situs and venous connections.
- The Environment: An abnormal axis with a structurally normal heart is not reassuring. Exclude thoracic masses and diaphragmatic hernia before concluding the scan.
References
- Comstock CH. Normal fetal heart axis and position. Obstet Gynecol. 1987;70(2):255-259. PMID: 3299186.
- Smith RS, Comstock CH, Kirk JS, Lee W. Ultrasonographic left cardiac axis deviation: a marker for fetal anomalies. Obstet Gynecol. 1995;85(1):97-102. PMID: 7824228.
- Shipp TD, Bromley B, Hornberger LK, Nadel A, Benacerraf BR. Levorotation of the fetal cardiac axis: a clue for the presence of congenital heart disease. Obstet Gynecol. 1995;85(1):97-102. PMID: 7800334.
- Carvalho JS, Allan LD, Chaoui R, et al. ISUOG Practice Guidelines (updated): sonographic screening examination of the fetal heart. Ultrasound Obstet Gynecol. 2013;41(3):348-359.
- McBrien A, Sonesson SE, Bhide A, Towers C, Murdoch E. Changes in fetal cardiac axis between 8 and 15 weeks’ gestation. Ultrasound Obstet Gynecol. 2013;42(6):653-658. PMID: 23640645.
- Zhao Y, Edington S, Fleenor J, et al. Fetal cardiac axis in tetralogy of Fallot. Ultrasound Obstet Gynecol. 2017;50(1):58-62.
- Wolter A, Kawecki A, Stressig R, et al. Fetal cardiac axis in fetuses with conotruncal anomalies. Ultraschall Med. 2017;38(2):198-205.
- Comstock CH, Smith RS, Lee W, Kirk JS. Right fetal cardiac axis: clinical significance and associated findings. Obstet Gynecol. 1998;91(4):495-499.
- Gembicki M, Wolter A, Glockner S, et al. Semi-automatic measurement of fetal cardiac axis in fetuses with CHD with FINE. J Clin Med. 2023;12(19):6371. PMC10573854.
