What is congenital heart block?
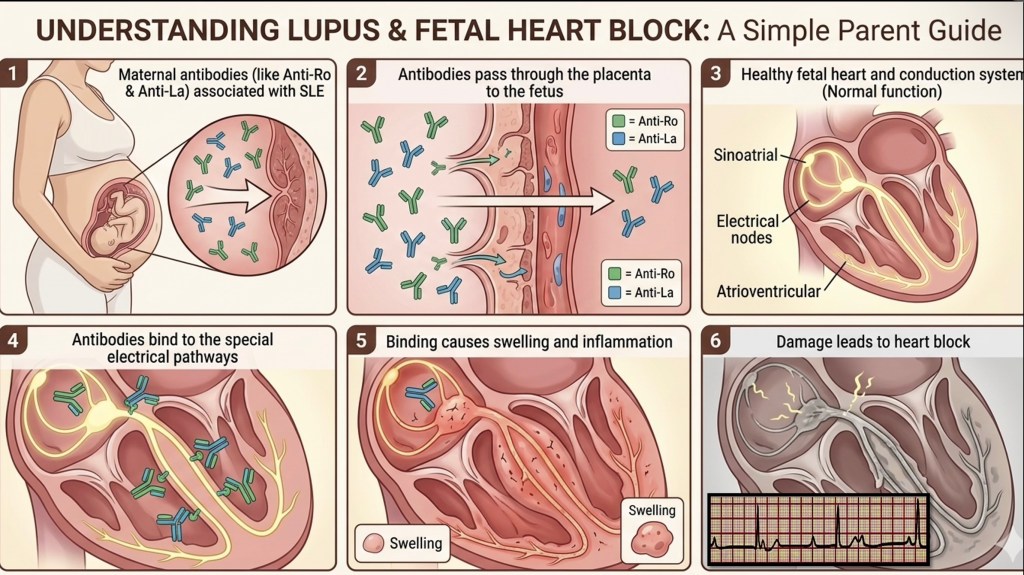
The heart has an electrical system that controls its rhythm. Congenital heart block means that the electrical signal between the upper and lower chambers of the heart is interrupted or delayed. In its most severe form, this can slow the baby’s heart rate significantly and may require a pacemaker after birth.
It is caused by specific antibodies, called anti-Ro and anti-La antibodies, which can cross the placenta and affect the developing cardiac conduction system, usually between 18 and 28 weeks of pregnancy.
How common is this?
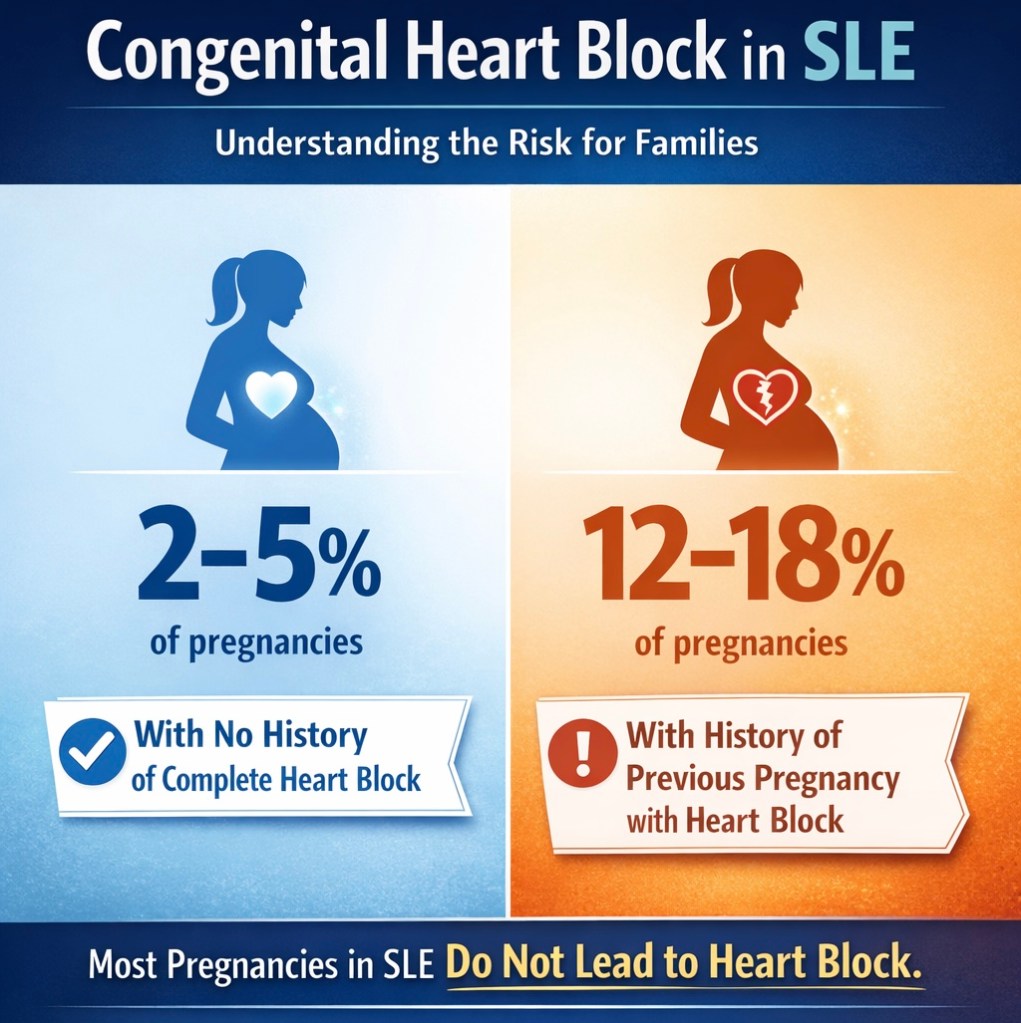
Not all women with SLE carry anti-Ro or anti-La antibodies. If you do carry these antibodies, the risk of complete congenital heart block in any individual pregnancy is approximately 2-5 percent. If a previous baby was affected, the recurrence risk rises to around 12 to 20 percent.
These numbers mean that the majority of women with SLE, even those with anti-Ro or anti-La antibodies, will have babies with completely normal heart rhythm. But the minority who are affected need early detection.
What Steps Should You Take After an SLE Diagnosis During Pregnancy?
Once a diagnosis of Systemic Lupus Erythematosus (SLE) is confirmed, the next important step is to test for anti-Ro and anti-La antibodies, if this has not already been done. Testing for these antibodies, preferably including their levels, is crucial in helping to assess the potential impact on the developing baby.
Pregnant women diagnosed with SLE should begin treatment with Hydroxychloroquine (HCQ), as this medication has been shown to reduce the risk of neonatal complications related to SLE.
It is recommended to consult with a rheumatologist to evaluate how SLE may be affecting the mother’s health. Additionally, obtaining an opinion from a pediatric or fetal cardiologist is important, and a fetal echocardiogram should be performed to thoroughly assess the baby’s heart.
What monitoring is recommended?
If you carry anti-Ro or anti-La antibodies, regular fetal cardiac monitoring between 16 and 28 weeks is recommended. This typically involves fetal echocardiography with Doppler assessment of the PR interval, which is a measurement of the electrical conduction time in the baby’s heart.
Early detection of first or second degree heart block allows for discussion of treatment options, including medications that may slow progression in some cases.
What about the rest of the heart?
Beyond the conduction system, a full structural fetal echocardiogram is also recommended for women with SLE to look at the overall anatomy of the heart. SLE is one of the established indications for fetal echo.
If you have SLE and are planning or currently in a pregnancy, we are happy to discuss your specific situation and what monitoring is appropriate for you.
