In this write-up, it has been tried to answer common quarries after diagnosis of ICEF on sonography with the facts and studies available. Most of the time, personal statements and opinions are given with either completely ignoring the finding or giving too much importance to it. There is a conclusion at the end summarising the result. To oversimplify, ICEF is of significance in very few pregnancies.
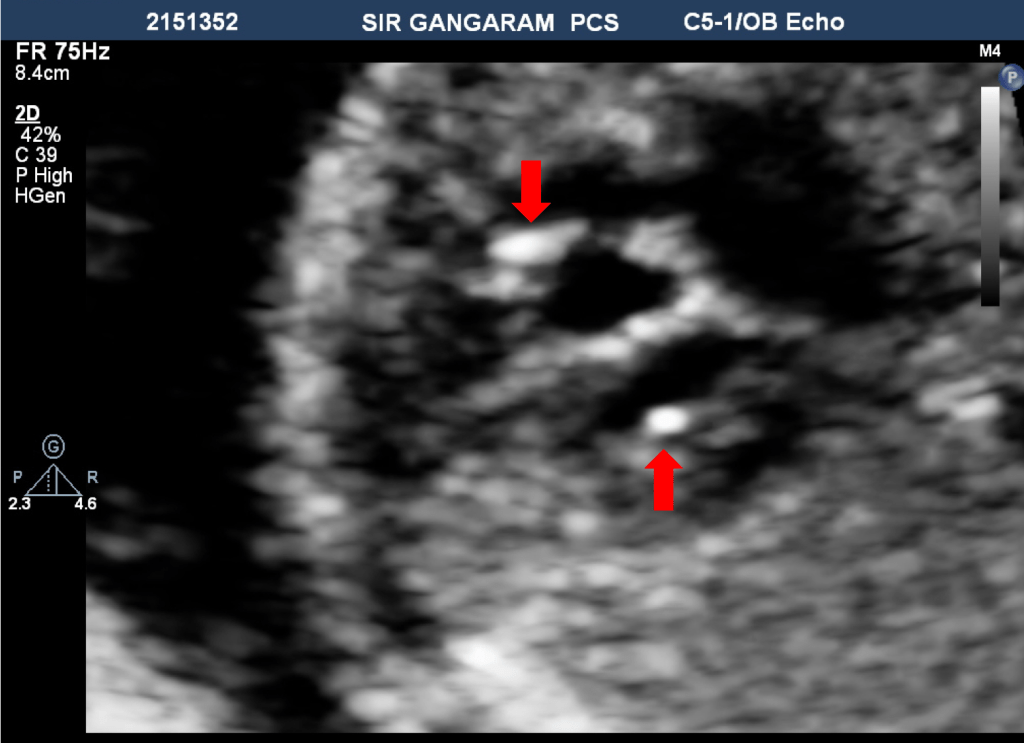
ICEF (sometimes called as Left ventricle Echogenic Focus-LVEF) is a sonographic finding of circumscribed focus that is ‘as bright as a bone,’ present in ventricle cavity, suggesting probably calcium deposition at papillary muscle or chordal attachment.
An EIF is defined as a small (<6 mm) echogenic area in either cardiac ventricle that is as bright as the surrounding bone and visualized in at least 2 separate fetal echo planes.
The prevalence of ICEF is reported between 2.3 to 9.6 % in various studies with slight higher in Asian population in few studies. Also, the prevalence is slightly higher in the maternal age group of >35 years as compared to <35 years. ICEF most commonly present in the left ventricle (up to 80% of all ICEF), followed by both ventricles (11-12%) and rarely in the right ventricle (3-4%). Sometimes multiple ICEF can be present in the same ventricle as well.
When ICEF is the only positive finding during a sonogram it is called ‘Isolated’ ICEF.
Association with Downs Syndrome
It has been reported that the prevalence of ICEF in fetuses with Downs syndrome is about 16% and of isolated ICEF is <5% in a centre with quality sonography services are available.
In studies where age stratification has not been done the sensitivity of isolated ICEF to detect Trisomy is between 4-11% and likelihood ration between 1.6 -2.8. A study where the maternal age is divided between 18-35 years and > 35 years, no case of Trisomy reported in 18-35 years age group (out of 192 ICEFs).
So, the conclusion could be Isolated ICEF in a low-risk group has a low chance of being Trisomy, but slightly higher in a higher risk group, and the further genetic evaluation can be based on it. Since the rule is not absolute, the counseling of involved should be done, and if they insist on further evaluation, the genetic testing can be offered after explaining the risk of the procedure as well.
Association with Congenital Heart Disease (CHD)
ICEF, as a detection tool for CHD, has shown a sensitivity of 1.5% in one study, whereas the prevalence of CHD with ICEF has been reported between 1.6- 4.2 % (the prevalence of CHD in the general population is about 0.8%). A study has reported an association between the location of ICEF and prevalence of CHD, with significantly higher with RV ICEF (14%) as compare to LV or biventricular ICEF (2.8 & 2.3%). This is the most common reason to opt for fetal echo after detection of ICEF on sonography.
What happens to ICEF?
ICEF itself is not a disease and do not affect the cardiac function or otherwise and expected to fade of during fetal, neonatal or sometimes later childhood. Neonatal echo is not necessary and should be offered if CHD was suspected or optimum imaging was not possible due to poor echo images.
Need for Fetal Echocardiography
There is no uniform guidelines to recommend Fetal echo when ICEF is diagnosed. However we follow our standardized protocol for a patient referred for consultation for ICEF.
- Determine if the patient is high risk or low risk, depending on maternal age, history of chromosomal defect or CHD or other organ system defect or presence of RV ICEF.
- If high risk the Fetal echo recommended.
- Low risk, then counselled that the risk of having heart disease is almost similar to general population, but Fetal echo can be opted if want to rule out CHD with certainty.
- Optional Neonatal echo should be offered to all with ICEF, with more emphasis to with high risk factors.
As there is a lot of variation among the studies for an association of ICEF with Trisomy or CHD, the counselling becomes very important. Involvement of various specialties and further imaging should help to rule out associations and to alleviate the anxiety, and in current prevailing medico-legal scenario it is a good idea to document all the counselling.
Conclusion
ICEF is sonographic finding showing a bright spot in the heart cavity, possibly calcium deposition. Chances of trisomy (Downs syndrome) with a low-risk group is low and in the absence of any other finding related to trisomy, is of little significance. In the presence of other risk factors, the finding of ICEF should be evaluated.
