
Aortic Arch Visualization in Fetal Echocardiography
In fetal echocardiography, a detailed sonographic evaluation of the great arteries is essential, particularly when assessing fetuses with potential arch anomalies or pulmonary slings. To ensure a comprehensive examination, several critical anatomical features should be carefully assessed (Wang and Zhang et al.):
- Origin of the Bilateral Pulmonary Arteries: Determine the presence and where the right and left pulmonary arteries originate from the main pulmonary trunk.
- Arch Laterality Relative to the Trachea: Assess whether the aortic arch is positioned to the trachea’s left or right (or both sides).
- Sidedness of the Ductus Relative to the Trachea: Evaluate the location of the ductus arteriosus concerning the trachea and arch.
- Presence of a Vessel Behind the Trachea: Check for any vessels positioned posterior to the trachea.
- Aortic Arch Branching Patterns: Examine the branching pattern of the aortic arch.
- Sidedness of the Proximal Descending Aorta: Note the position of the proximal descending aorta relative to the midline, which is crucial for identifying arch anomalies.
A comprehensive understanding of these aspects can be obtained through serial transverse scans. By continuously moving the ultrasound probe cephalad along the fetal thorax’s vertical axis, a detailed anatomical assessment is possible.

The Three-Vessel and Trachea (3VT) View
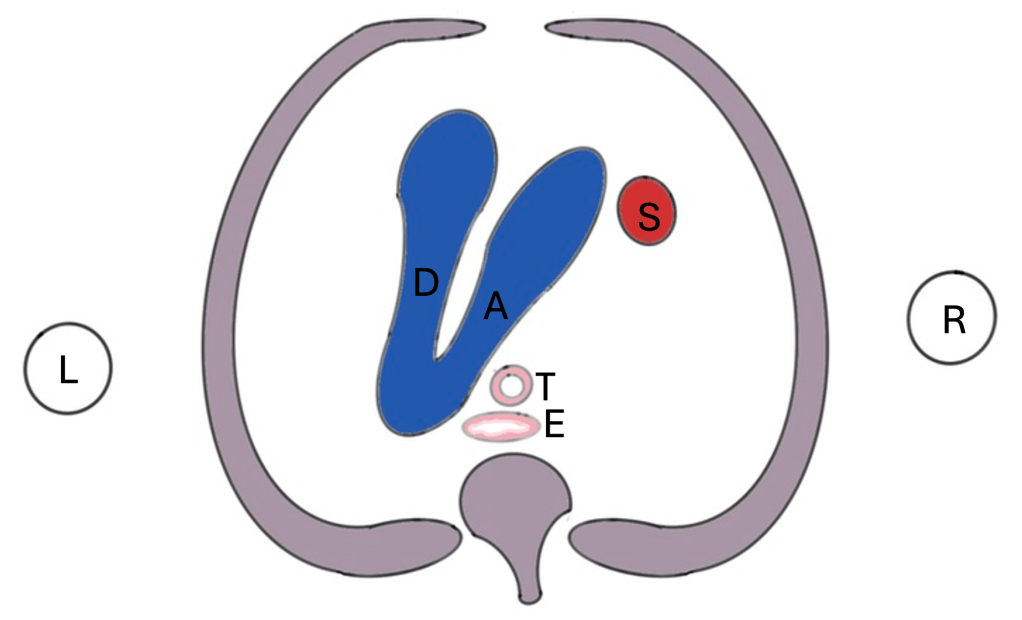
The three-vessel and trachea (3VT) view is a critical perspective in fetal echocardiography. It is obtained when the ultrasound beam crosses the junction of the aortic arch and ductus arteriosus. This view typically forms a “V” shape with the trachea and the superior vena cava (SVC) positioned on the right, which is indicative of a left aortic arch with a normal branching pattern.
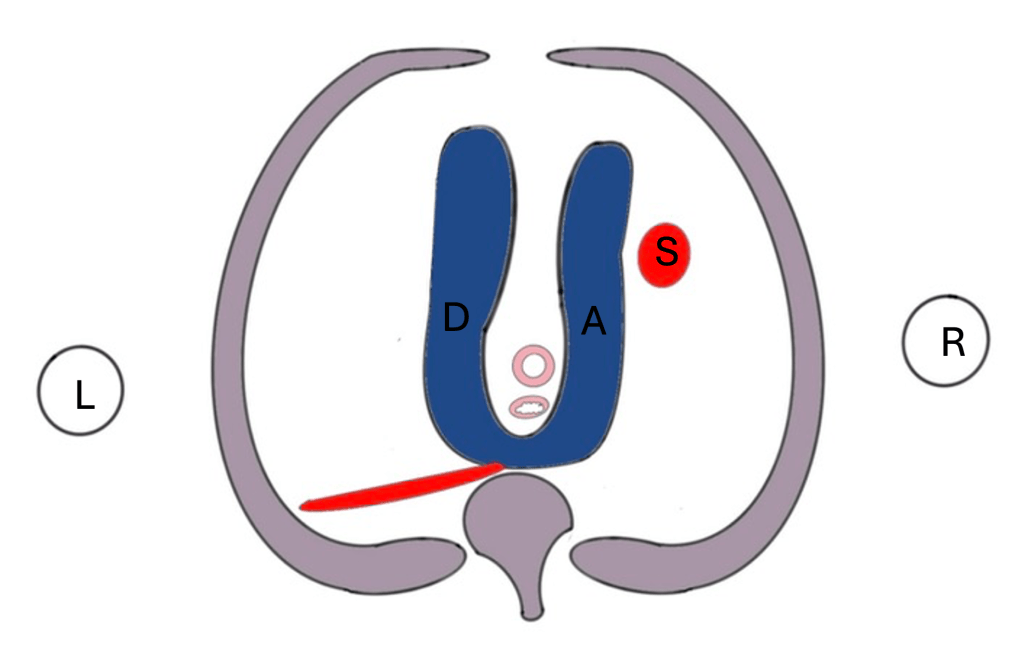
However, variations in this pattern can reveal different arch configurations. For instance, a “U” shape on the 3VT view may suggest an abnormal arch pattern. The goal of examining the V and U patterns within the 3VT view is to diagnose common arch anomalies. Additionally, incorporating a coronal view (Y connection) can provide further diagnostic clarity in some cases.

The V pattern

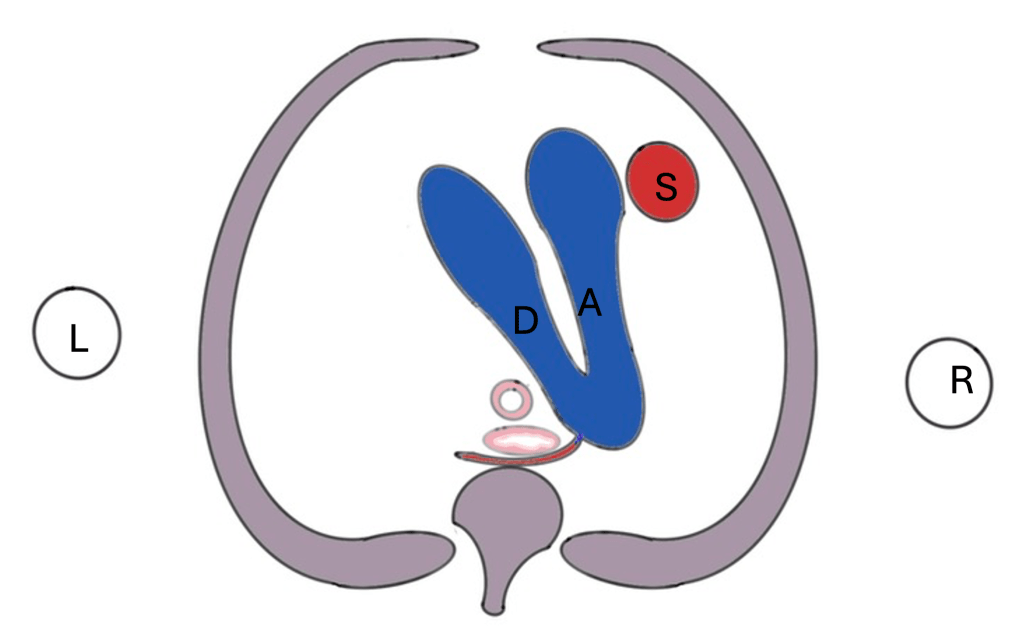
The U pattern



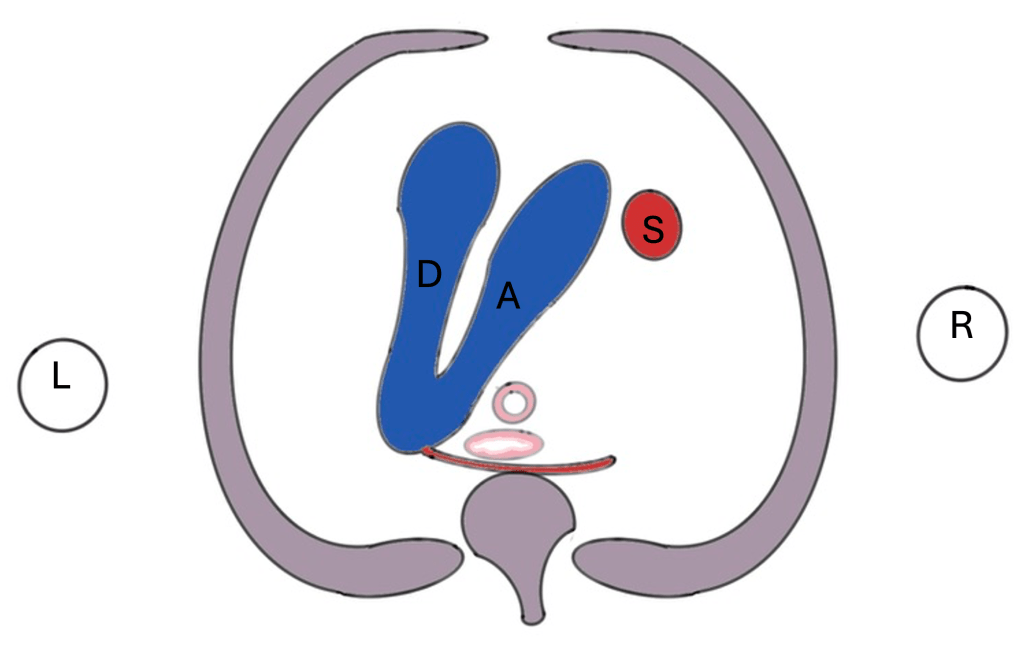
Coronal Plane Views (The “Y”)
The coronal plane section through the proximal descending aorta provides another essential view. It effectively demonstrates the junction between the arch and the descending aorta and can reveal the presence and trajectory of an aberrant left or right subclavian artery. When tracing a suspected aberrant subclavian artery, it is crucial to follow its distal path and the direction of blood flow to differentiate it from the ductus arteriosus. The coronal Y pattern can confirm the presence of subclavian aberrancy rather than serving as the primary diagnostic tool.
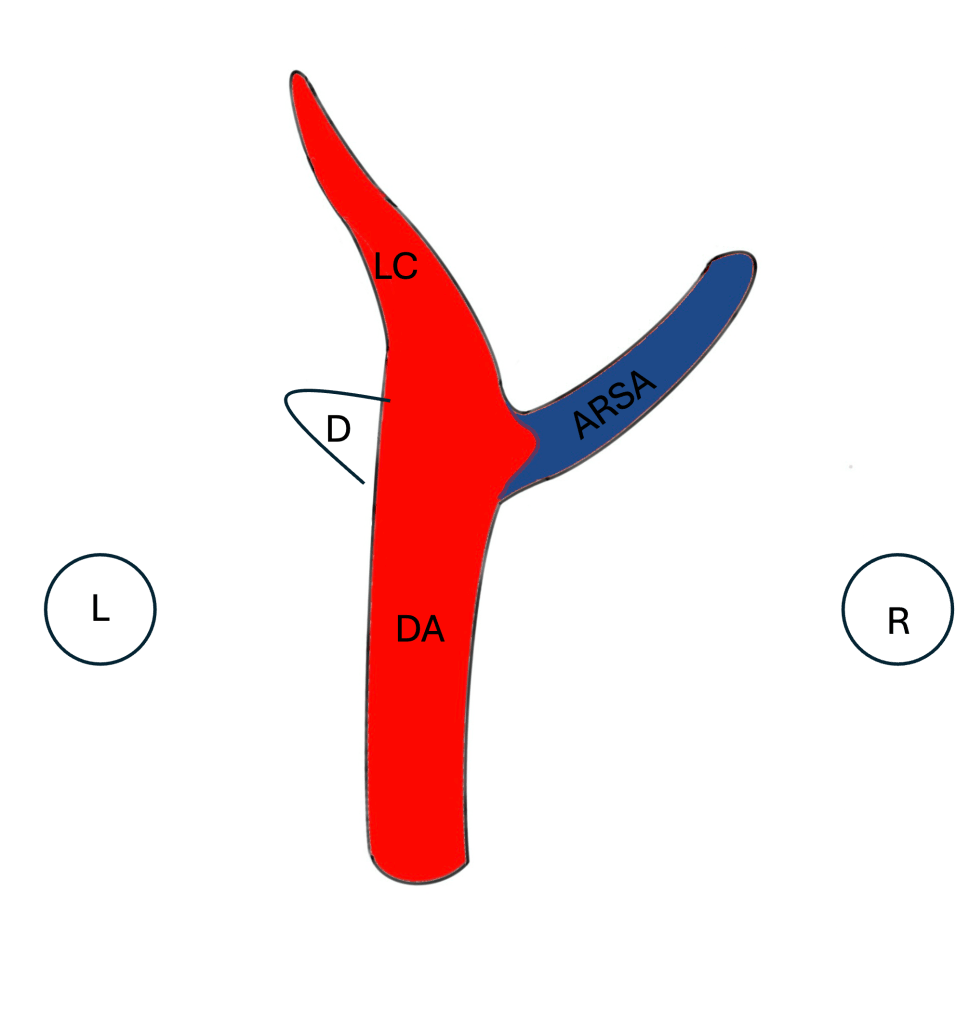
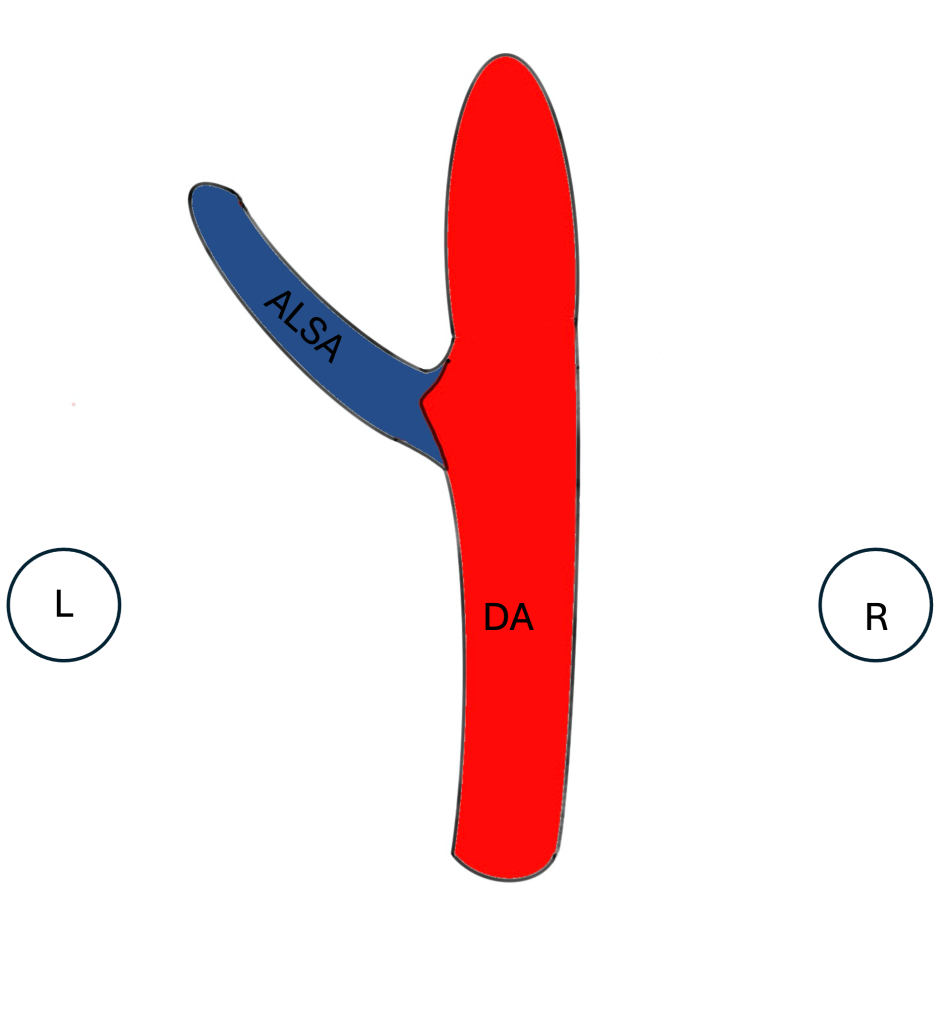
(ALSA), DA-Descending Aorta, L- Left of Fetus, and R- Right of Fetus


Long-Axis Views
The long-axis view of the aortic arch is particularly valuable for visualizing the continuous pathway of the ascending aorta, aortic arch, and descending aorta. This perspective also allows clinicians to pinpoint the origins of the head and neck branches, which is critical for understanding the anatomy in cases of suspected anomalies.
Other Anomalies
This write-up focuses on the most common types of aortic arch anomalies but is not exhaustive. Notably absent are the circumflex aorta and pulmonary artery sling, both of which also present a “U” pattern. Additionally, a right aortic arch with a left ductus continuing with a left innominate artery does not form a “U” pattern and is not covered here.
Conclusion
By meticulously assessing these anatomical features using the appropriate sonographic planes, healthcare providers can achieve a comprehensive evaluation of the great arteries in both normal fetuses and those with potential arch anomalies. Mastery of the V, U, and Y patterns in fetal echocardiography not only aids in accurate diagnosis but also enhances our understanding of congenital heart defects, ultimately improving fetal outcomes.
