Umbilical–Portal–Systemic Venous Shunt (UPSVS) define as abnormal communication between umbilical vein, portal venous system or ductus venosus with hepatic vein, systemic vein, or to a cardiac structure (RA, LA, CS).
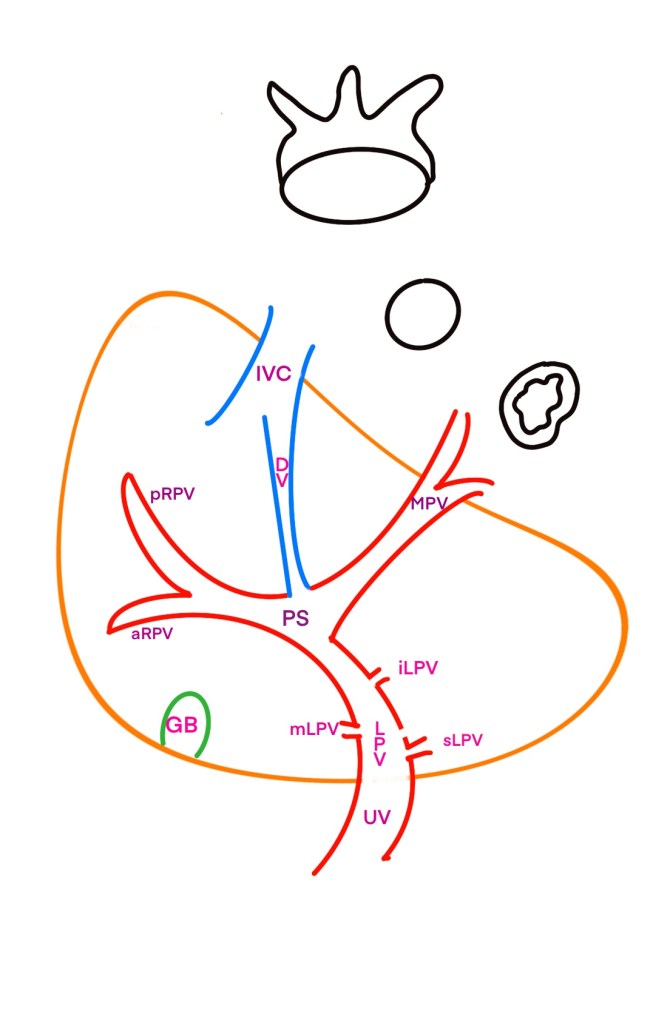
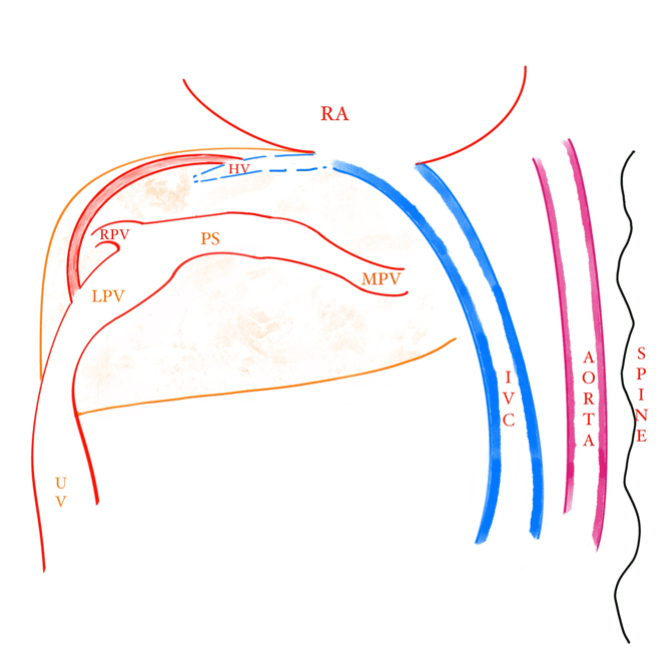
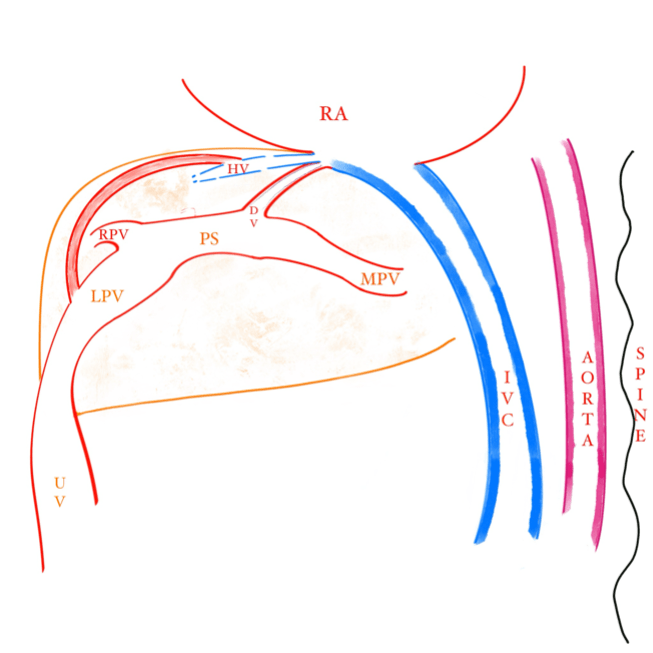
Normal Umbilical portal system
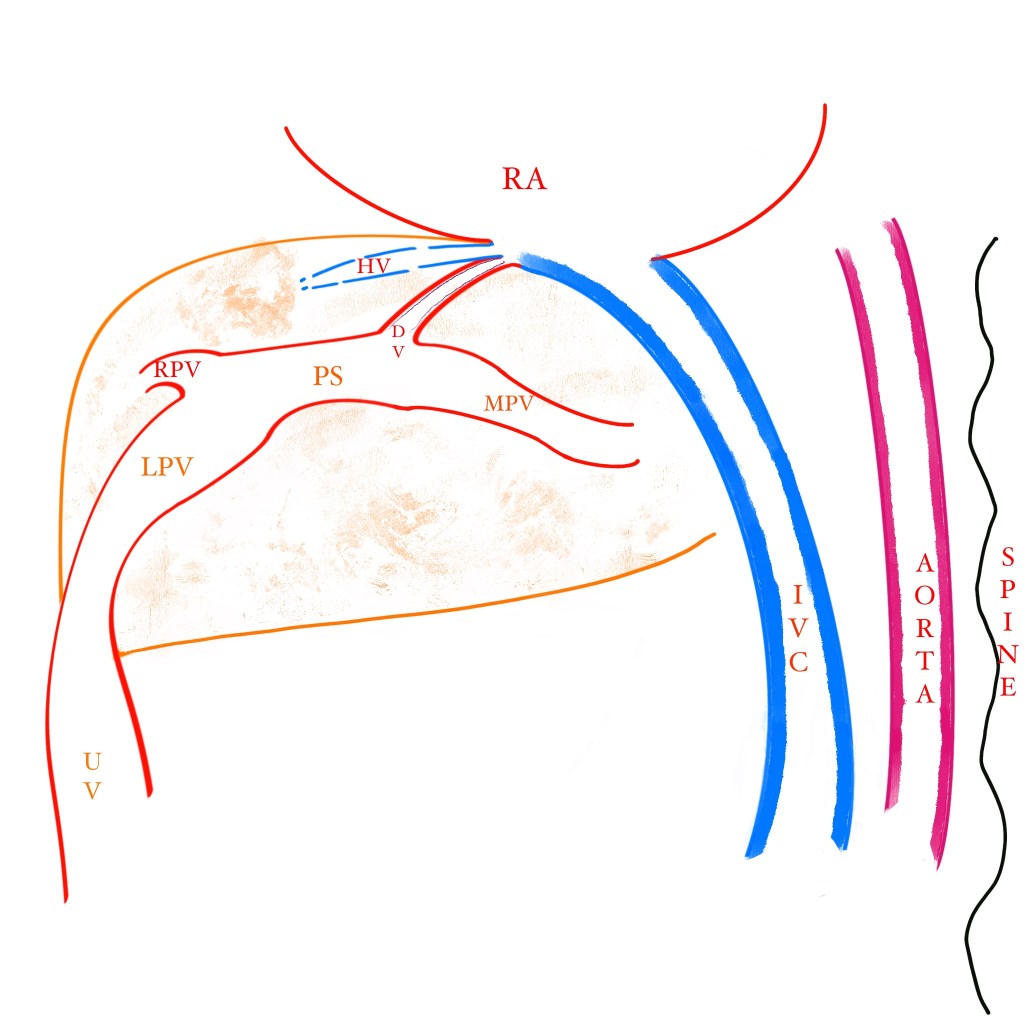
The ‘left’ umbilical vein (UV) enters the fetal abdomen at cord insertion and connects to left portal vein (LPV). LPV gives three branches to the left lobe of the liver, superior, middle and inferior. LPV then continues as portal sinus (PS).
Portal sinus (PS) is the vascular space extending from the point of origin of the inferior branch of the left portal vein to that of the right portal vein (RPV) branches into right anterior and posterior PVs. PS gives rise to ductus venous (DV) and then turns to right where it joins main portal vein (MPV).
DV drains into IVC along with three hepatic veins into the sub-diaphragmatic vestibulum at the base of the right atrium.
The classification and understanding of these shunts are essential for accurate prenatal diagnosis, management, and counselling of affected pregnancies
Summarized from:
Achiron R, Kivilevitch Z. Fetal umbilical-portal-systemic venous shunt: in-utero classification and clinical significance. Ultrasound Obstet Gynecol. 2016 Jun;47(6):739-47. doi: 10.1002/uog.14906. PMID: 25988346.
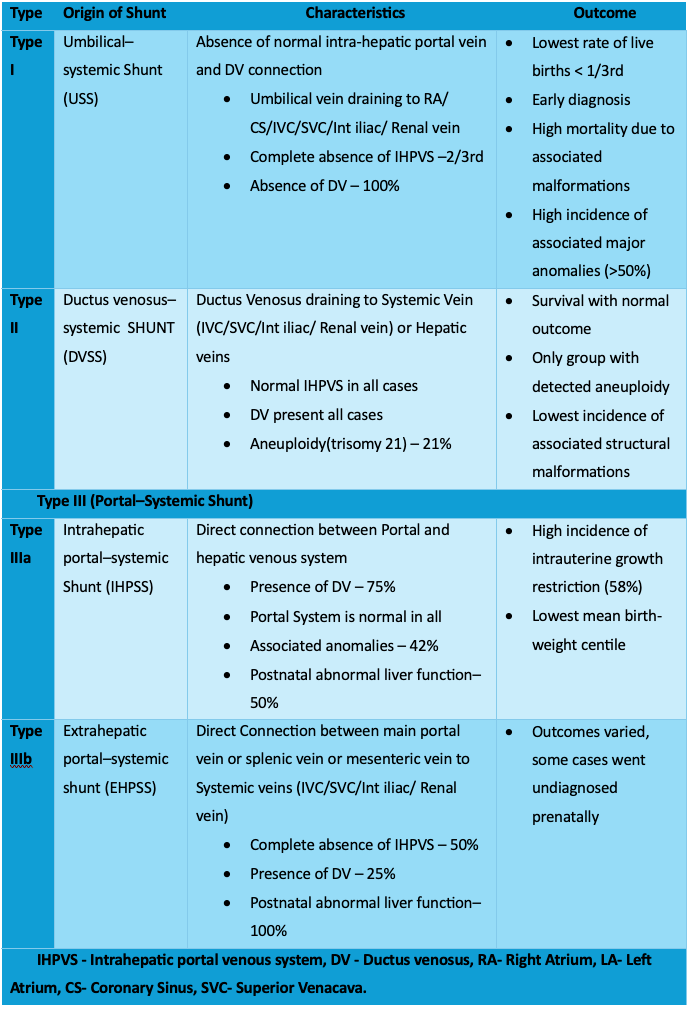
The distinctive feto-maternal clinical characteristics and outcomes associated with each type of shunt:
- Type I had the earliest diagnosis, a high incidence of associated anomalies, and the lowest live birth rate.
- Type II had a wholly intact IHPVS, a notable rate of aneuploidy, and a low frequency of structural malformations.
- Type III had varying outcomes with some cases showing growth restriction and others requiring postnatal surgery. 50% of III b have complete absence of IHPVS and overall half of IIIa and all of IIIb had abnormal liver function tests.
Absent Ductus Venosus (ADV)
| Type | Origin of Shunt | ADV % |
| Type I | Umbilical–systemic Shunt (USS) | 100% |
| Type II | Ductus venosus–systemic SHUNT (DVSS) | 0% |
| Type III (Portal–Systemic Shunt) | ||
| Type IIIa | Intrahepatic portal–systemic Shunt (IHPSS) | 25% |
| Type IIIb | Extrahepatic portal–systemic shunt (EHPSS) | 75% |
The ultrasound features for each type of fetal umbilical–portal–systemic venous shunts are as follows:
Type I (Umbilical–systemic shunt, USS):
- The umbilical vein fails to connect normally with the left portal vein and ductus venosus.
- In some cases, the UV courses directly to the right atrium or is connected to the systemic circulation via other pathways such as the inferior vena cava or iliac vein.
- The intrahepatic portal venous system may be absent or only partially present.
- The DV is not visualized in these cases.
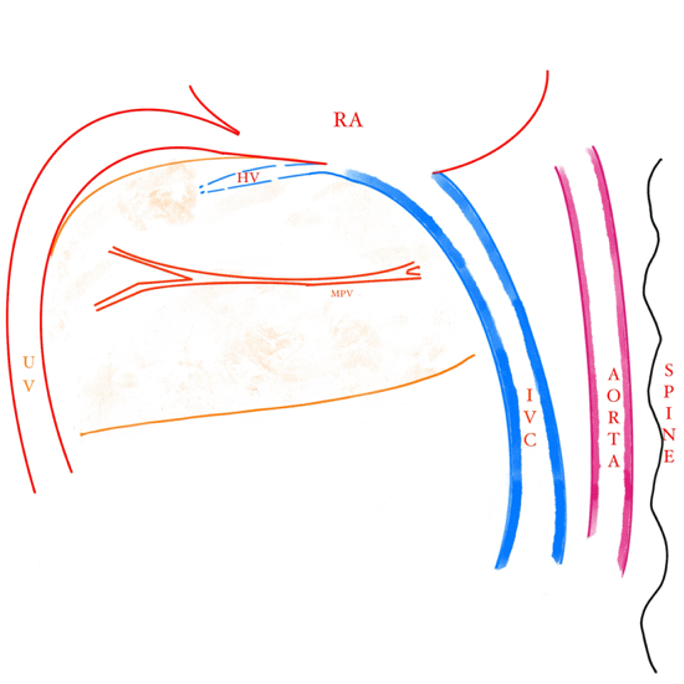
Type II (Ductus venosus–systemic shunt, DVSS):
- The normal umbilical–portal–DV complex is present, but the blood flow in the DV is shunted into the systemic circulation instead of its normal path toward the left heart.
- Cases may show a downward displacement of the umbilical–portal–DV complex into the inferior vena cava, with a vertical end-to-side anastomosis.
- The hepatic vein may also drain into the IVC, situated below the pre-diaphragmatic infundibulum.
- A normal IHPVS is present in all cases of DVSS.

Type III (Portal–systemic shunt):
This group is further divided into intrahepatic and extrahepatic subtypes based on the location of the shunt.
Type IIIa (Intrahepatic portal-systemic shunt, IHPSS):
- Unilateral shunts may be found between a branch of the portal vein and a hepatic vein.
- The IHPVS may be observed intact or with segments absent.
- End-to-end or cavernous anastomoses may be present.
- The DV may be absent in some cases
Type IIIb (Extrahepatic portal-systemic shunt, EHPSS):
- Abnormal connections may occur between the main portal vein or splenic vein and systemic veins such as the IVC, bypassing the liver.
- There can be a mixed shunting pattern involving umbilical and portal vessels.
- Potentially absent intrahepatic portal venous system or significantly hypoplastic, impacting the portal flow into the liver.
- Direct side-to-side connections can be identified between the main portal vein and vessels like the inferior vena cava, sometimes proximal to a short ductus venosus.

The various types of UPSVS may present with specific ultrasound features, which can help in differentiating between them.
Long-term follow-up is critical for monitoring infants with these anomalies to capture any delayed complications, such as growth and developmental delays or further vascular changes.
Conclusion
In conclusion, differentiation between the types of shunts enhances our understanding of their unique anatomical configurations and potential clinical outcomes.
Type I shunts(USS) demonstrated the lowest live birth rate and high associated morbidity due to prevalent anomalies, whereas Type II (DVSS) shunts, with intact intrahepatic portal venous systems, showed a better prognosis and lower incidence of structural malformations. Type III (EHPSS & IHPSS) shunts had more variable outcomes, with particular attention to the potential long-term liver function implications.
The presence of the intact intrahepatic portal venous system has emerged as a favorable prognostic factor, underscoring the importance of its accurate prenatal assessment.
Future research should focus on the refinement of diagnostic techniques, ideally augmenting prenatal screening programs. This will aid in early detection and better prognostication of fetal UPSVS, thus allowing for more informed counseling of expectant parents and timely planning for postnatal care.
Moreover, understanding the genetic underpinnings and pathophysiological mechanisms involved in the development of UPSVS could pave the way for advancements in preventative measures and therapeutic options.
